VANDANA REDDY
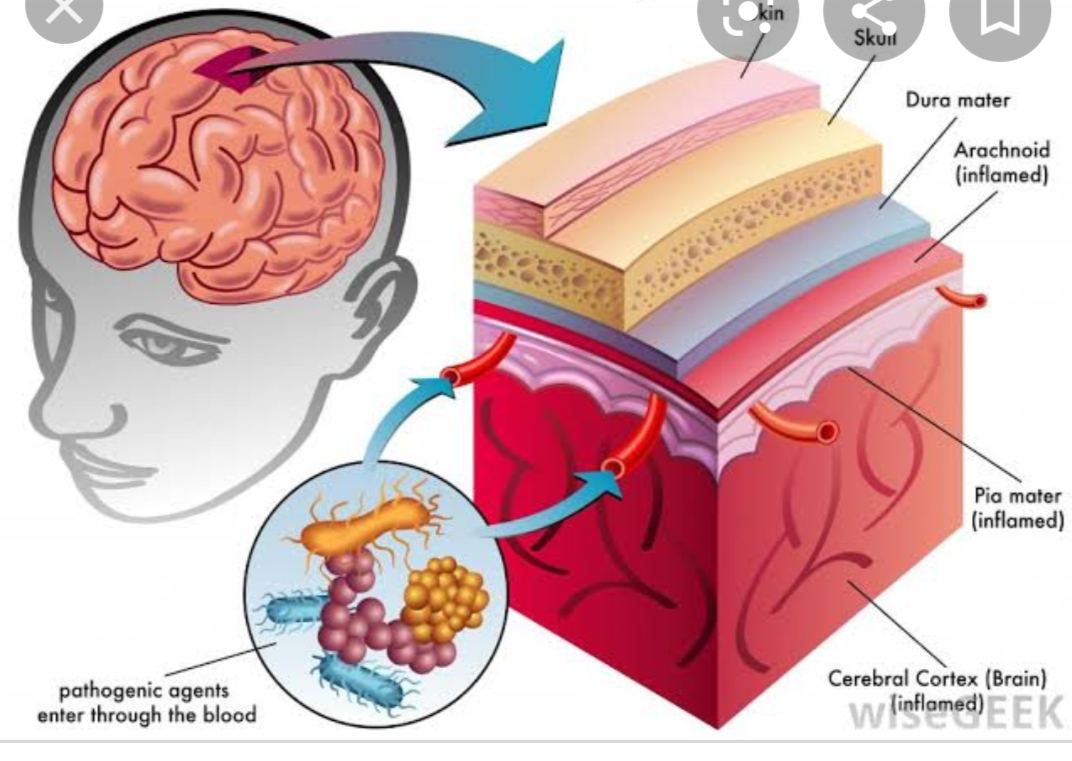
BIMONTHLY INTERNAL ASSESSMENT FOR THE MONTH OF JANUARY 2021 January bimonthly assessment exam 2021 26yr old women came with complaints of altered sensorium since 1 day,headache since 8 days,fever and vomitings since 4 days More here: https://harikachindam7. blogspot.com/2020/12/26-year- old-female-with-complaints-of. html Case presentation links: https://youtu.be/fz9Jssoc-mA https://youtu.be/d4lLX04oL8s https://youtu.be/CSCxw2zp7Oc a). What is the problem representation of this patient and what is the anatomical localization for her current problem based on the clinical findings? Pt has complaints since 1 month she has headache 1-2 times per week relieved on medication .but the headache worsened in the past 15 days ., c/o Heaeache since 8 days- in bitemporal vertex region has been aggrevated since 1 week . After stopping using steroids she has fever since 4 days- low grade not associated with chills and rigors. vomitings sin...